Please note that this summary was posted more than 5 years ago. More recent research findings may have been published.
Summary
The nature of patient needs and ward activity is changing. Inpatients tend to be more ill than they used to be, many with complex needs often arising from multiple long-term conditions. At the same time, hospitals face the challenges of a shortage and high turnover of registered nurses. This review presents recent evidence from National Institute for Health Research (NIHR)-funded research, including studies on the number of staff needed, the support workforce and the organisation of care on the wards. While few research studies have explored the similar pressures that occur in community and social care, the learning from hospitals may be useful to decision makers in these areas.
Culture or climate? ‘Climate’ describes the shared perceptions people have about their workplace while ‘culture’ refers to the beliefs, values, and assumptions that direct the behaviours of an organisation.
Shaping the team: size and mix
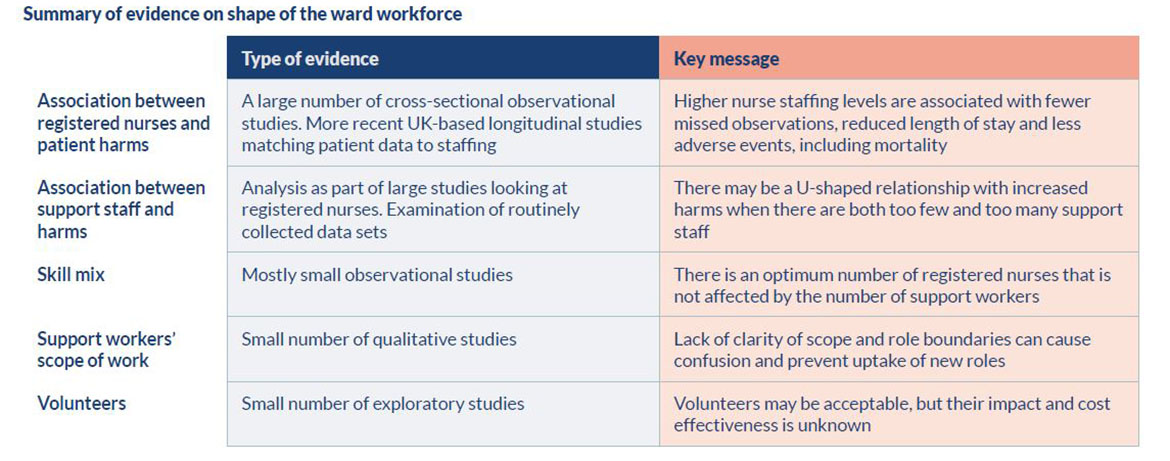
Making decisions about optimal ward staffing is complex. There is a large body of evidence, including recent UK research, demonstrating a positive relationship between the number of registered nurses in hospital wards and patient safety. The evidence suggests the relationship is not linear and we don’t yet understand enough to determine the optimum staffing levels in individual wards. NIHR studies are shedding more light on the factors that decision makers need to take into consideration.
A number of NIHR studies have looked at different support roles and identified lack of clarity around role boundaries. Research suggests that the contribution of registered nurses is distinct from that of healthcare assistants or support workers. However, the roles do overlap and the issue of how work should be distributed needs careful consideration.
Other studies have looked at the way in which nurses work with other professions to provide care on the ward and the importance of ward leadership. Research suggests emerging roles will need careful evaluation to assess their impact on care delivery and quality.
Managing the team and the ward
Planning the shape of the team is critical but managing wards well is not just a numbers game. Managers need time and training to manage staff and to use roster planning tools well. Evidence is emerging that patient experience is affected by staff wellbeing and local ward climate. Teamwork, clear role design and good local leadership all contribute to positive ward environments.
Retaining staff is as important as recruiting new people. Whilst there is a lack of evidence on interventions to do this, contributory factors tend to be multifactorial and include non-pay rewards and practice climate.
The way work is organised can have a significant impact on efficiency. There have been many interventions to improve how ward work is organised but these are often poorly evaluated and may have unintended consequences. Improvement projects are widely used in hospitals and can be effective but need careful planning and staff education to ensure sustained impact.ich nurses work with other professions to provide care on the ward and the importance of ward leadership. Research suggests emerging roles will need careful evaluation to assess their impact on care delivery and quality.
As a non-professional in the management of the NHS Healthcare sector, I found this review informative and well supported with evidential resources. As a result I now feel I have a greater understanding of the issues of ward staffing than before.
Ron Capes, Lead Governor, Basildon and Thurrock University Hospitals NHS Foundation Trust
Introduction
In 2016 the NHS spent £73.8 billion on hospital services (ONS 2016), with staffing accounting for 70% of the costs (Dixon et al. 2018). Across the NHS, registered nurses and midwives make up 26.8% of all staff with healthcare support staff making up a further 15% (NHS Digital 2018a). We do not know exactly how many registered nurses and support staff work on hospital wards, but they make up a significant part of the overall hospital spend.
NHS hospitals have to balance staffing levels needed to deliver care that is safe and effective with the constraints of finite funding. New roles and changing relationships between professional groups can potentially help or hinder that balance, as can the way ward staff are managed. Research evidence can help managers to make informed and risk-based assessments about the ward workforce.
Aim and scope of the review
The aim of this review is to be informative and accessible. We provide a narrative that sets the scene through landmark studies, important new research and early work that is promising but needs further development. We hope decision makers, including senior nurses who plan and manage ward staffing on a day-to-day basis, human resource professionals, hospital managers and hospital boards and the public will find it helpful. Questions have been identified at the end of each section for organisations as a prompt to review their practice.
Our starting point for this review is research from the NIHR. This is the largest government funder of health research in the UK and includes dedicated programmes and projects on the organisation and quality of care. Working with clinicians, patients and managers, the NIHR has identified gaps in knowledge and funded new research on nurse staffing, clinical teams and improving care on hospital wards. Guided by our expert steering group, we have also included selected landmark international studies and UK-based research of interest to readers. Studies that were funded by the NIHR are identified by letters of the alphabet and a summary of each study can be found in the appendix. Other, non-NIHR, studies are cited by author name and full references given at the end of the review.
This is not a systematic review and is in part directed by the NIHR research studies available to us. We recognise the shift in policy towards healthcare provided outside of hospital and in adult social care but, at present, there is a shortage of research evidence on staffing in these areas. Hospital ward staffing remains an important issue and this review focuses on staffing within 24-hour care inpatient facilities designed to provide health rather than social care. While the available evidence is mixed in terms of research strength and generalisability, we recognise ward staffing still needs to be managed and the service cannot wait for the perfect study. Thus despite a degree of uncertainty in the evidence, we have included both large and small studies that inform decision making, including those with promising findings that need further exploration.
We describe the broad state of the evidence and highlight three NIHR-funded studies to provide more depth. We start with a background section which describes the current workforce challenges and what we know of ward staffing today.
Understanding Ward Staffing
Making decisions about ward staffing is complex. There is strong evidence linking the number of registered nurses to the rate of patient harms, including mortality. Whilst important as measures of safety, harms and mortality may not be the most sensitive indicators of adequate ward staffing. People are more than just their illnesses. The way we deliver care influences the experience of care as well as clinical outcomes. Nurse staffing has been shown to be associated with patient satisfaction as well as physical outcomes (Aiken 2018, Griffiths et al. 2018).
Ball et al. (2014) found that when staff were pressed for time, they were most likely to miss activities such as comforting, talking with and educating patients. The RN4cast study showed a link between the level of missed care and patient experience (Bruyneel et al. 2015) as well as outcomes (Ball et al. 2017). Good patient experience is positively associated with clinical effectiveness and patient safety. Doyle et al.’s (2013) review found consistent positive associations between patient experience, patient safety and clinical effectiveness across a wide range of diagnoses and care settings.
We see health systems around the world struggling with increasing demand and challenges in workforce supply. Patient safety has moved to the centre of policy and operational decision making and that means significant attention is being paid to safe nurse staffing. There are some striking core findings from across the evidence that all countries should consider, in particular the importance of nurse leadership.
Howard Catton, Chief Executive, International Council of Nurses
Providing the right number of staff is made harder when the supply of potential staff is failing to meet demand. Buchan et al. (2017) examined nurse numbers and pay policy in the UK in relation to the long term sustainability of the NHS, concluding that transformation will not be achievable without a serious examination of the way the NHS plans and uses the nursing workforce. Workforce forecasting to ensure adequate numbers of new entrants to the professions is critical, as is providing the conditions that retain experienced staff.
NHS Improvement (who license NHS providers in England) reported registered nurse vacancies as 41,772 in June 2018 out of 317,884 posts (NHS Digital 2018b). The Royal College of Nursing’s analysis show that, far from filling this gap, the supply of registered nurses will decrease over the next five years (RCN 2018). These challenges are not unique to the UK. The World Health Organisation (WHO) estimates that nurses and midwives represent more than 50% of the current shortage in health workers globally and that the world will need an additional 9 million nurses and midwives by the year 2030 (WHO 2018). This means that overseas recruitment may be increasingly difficult.
Increased access routes to becoming a registered nurse include a new type of worker, the Nursing Associate, which will be regulated by the Nursing and Midwifery Council from February 2019. The role is designed to be both a stand-alone role and to provide a progression route into graduate level nursing. It is likely that some trusts will review their skill mix to incorporate this role.
Alternative preparation for becoming a registered nurse in the UK
- Three year undergraduate nursing degree
- Two year post graduate nursing degree
- Four year nursing apprenticeship degree (since 2017)
- Two year apprenticeship Nursing Associate (a new registered role from 2019) who can then study for a further two years to gain a nursing degree
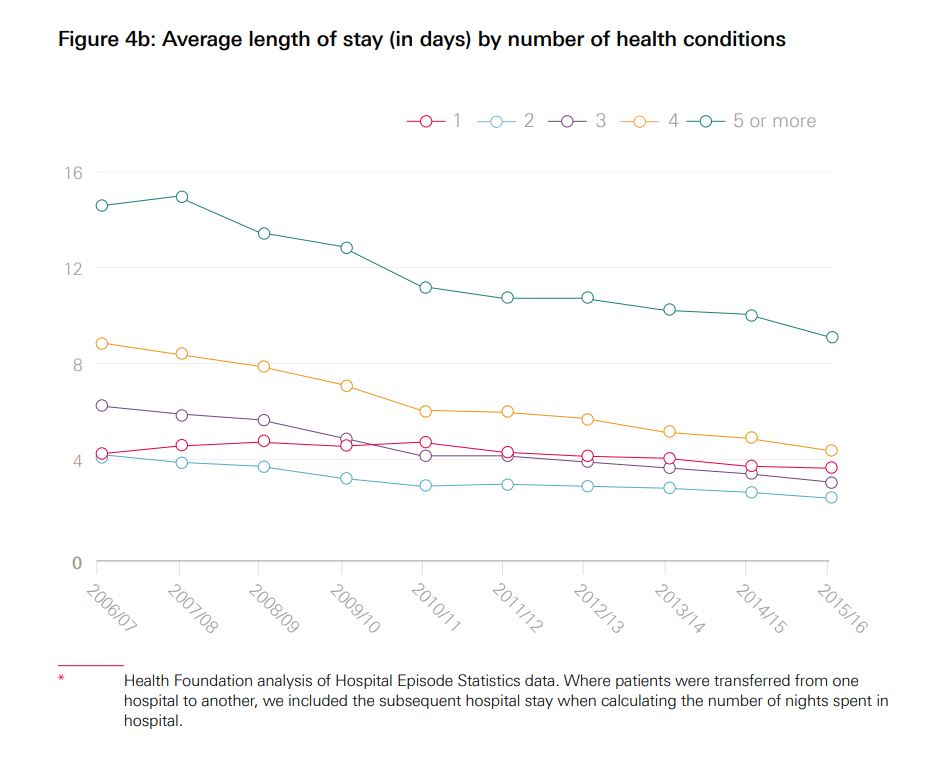
Demand for inpatient care is changing. More healthcare is delivered without an inpatient stay (e.g. day case surgery) and inpatients are having shorter lengths of stay. This means people in wards may be more acutely unwell than ever before. An increasingly ageing population, with multiple long-term comorbidities means more care is being delivered out of hospital. When people do need to be admitted to hospital, they often need more support with activities of daily living than inpatients needed in the past. On the other hand, pressures on adult social care and community services can mean some people with complex needs staying in acute hospitals longer than needed for their clinical care. Whilst they are less acutely ill, they may still need intensive help with fundamental care and ward staff may need to provide skilled rehabilitation care once their acute problems have been resolved.
Care in wards is provided by a combination of staff. A number of professions, including medical staff, physiotherapists, occupational therapists and pharmacists together with their assistant practitioners (physician associates, pharmacist technicians and therapy support workers), social workers, psychologists and specialist nurses all provide valuable input. The majority of patient contact time in wards is currently delivered by registered nurses and unregulated care assistants. The challenge of designing studies that can measure the effects of staffing in a way that takes account of the complex relationships between these diverse staff groups means that there is a gap in the evidence on professional interdependencies and the extent to which the number of staff from different professions can impact on the overall skill mix required. As a result, most of the published evidence relates to the impact of registered nurses and healthcare assistants. Each of the four countries of the UK has taken a slightly different policy approach to guidance on ward staffing (see below) and professional judgement remains important, given the differences in the many variables affecting outcomes in local contexts.
Policy guidance on determining ward staffing in the UK - brief overview
England: The National Quality Board published guidance for the NHS in England. Trust Boards are expected to agree an annual strategic staffing review, using evidencebased tools, professional judgement and comparison with peers and in line with their financial plans.
Wales: The Welsh Nurse Staffing Levels Act places a duty on Health Boards and NHS trusts to calculate and maintain nurse staffing levels in adult acute medical and surgical inpatient wards.
Scotland: A Bill for an Act of the Scottish Parliament to make provision about staffing by the National Health Service and by providers of care services is currently under consideration.
Northern Ireland: The Department of Health, Social Services and Public Services published a framework of expected ranges of nurse staffing in specific specialities. Where nurse staffing is outside the normal range, the Executive Director of Nursing must provide assurances about the quality of nursing care to these patients.
Shaping the team
The relationship between ward staffing and patient outcomes: There is strong evidence showing a relationship between ward staffing and both patient and staff outcomes. International and UK-based researchers have examined large datasets and demonstrated statistical associations between the number of patients a registered nurse cares for and a number of clinical outcomes. Limitations occur when routinely collected data are analysed alongside nurse surveys, as lags in patient data availability mean that the two data sources are not always perfectly aligned and the individual patient data is not linked to real-time staffing. However, the sample sizes in these studies and the number of studies reproducing the same findings mean the findings cannot be overlooked. A recent NIHR study published in 2018 (Study A) addresses these limitations and provides new evidence supporting a relationship between higher levels of nurse staffing and better patient outcomes.
International research has established a relationship between nursing levels and quality of care. Aiken’s seminal 2002 cross sectional study of 10,184 staff nurses and 232,342 surgical patients in the US found that for each additional surgical patient assigned to a registered nurse the odds of death increased by 7%. Similarly, Needleman et al. (2002) used data from 799 hospitals in 11 states that showed that good care is associated with both skill mix (the proportion of registered nurses) and with the total number of registered nurse hours.
The RN4Cast team (http://www.rn4cast.eu/) explored whether these findings would be replicated in Europe by testing the American findings across twelve countries and obtained remarkably similar results (see below).
Featured Study A
Higher registered nurse staffing levels were associated with fewer missed observations, reduced length of stay and adverse events, including mortality.
The authors sought to address some of the limitations in the evidence base identified by NICE by linking data at the patient level and modelling the economic impact of changes in ward staffing. This was a retrospective longitudinal observational study in one hospital in the UK. Results showed that the relative risk of death was increased by 3% for every day registered nurse staffing fell below the ward mean. Missed observations in acutely ill patients were significantly associated with lower registered nurse hours (but not support worker hours) and this was stronger on medical wards than on surgical wards. Other types of missed care were related to combined registered nurse and support worker hours but not the skill mix. This study provides high quality evidence of the relationship between staffing levels and patient outcomes. It tests a hypothesised causal mechanism and moves away from simply showing cross sectional associations.
The RN4CAST study
The European Union funded the RN4CAST team to study hospital nurse recruitment, nurse retention and patient outcomes in 12 European countries: Belgium, England, Finland, Germany, Greece, Ireland, the Netherlands, Norway, Poland, Spain, Sweden, and Switzerland. The study was conducted across 488 hospitals.
Findings from the project relating to nine of the countries (including England) include:
- An increase in a nurse’s workload by one patient increased the likelihood of an inpatient dying within 30 days of admission by 7%
- Every 10% increase in the number of degree-educated nurses was associated with a decrease in the likelihood of death of 7%
The study looked only at patients undergoing common general surgery, not all patients. The authors also acknowledged that other unmeasured factors at the individual, hospital, and community level could have affected the results (Aiken et al. 2014).
Evidence to inform guidance on ‘safe staffing’ level: Following concerns raised by the public inquiry into Mid Staffordshire NHS Foundation Trust (known as the Francis report), the Department of Health and NHS England asked the National Institute for Health and Care Excellence (NICE) to develop evidence-based guidelines on safe staffing, with a particular focus on nursing staff. NICE commissioned two reviews of the evidence. The first by Griffiths et al. (2014) noted that the evidence was derived from observational studies in different countries, some of which had very different contexts and cost bases to the UK. Whilst the evidence is generally supportive of a positive relationship between staffing levels and outcomes, the fact that it is largely observational research means it is not definitive. Griffiths et al. concluded that the different contexts, outcomes, measures of staffing and methods of analysis used across the evidence made it difficult to identify safe staffing levels in the NHS with certainty.
The second review by Cookson et al. (2014) examined the cost-effectiveness of nurse staffing and skill mix on patient outcomes associated with nursing care and found only four economic studies of nurse staffing and patient outcomes, including one cost effectiveness study. None of the studies were from the UK nor did they use ward level data. The team therefore estimated effects using UK ward level data, but the poor quality of the available data limited generalisability. Neither review rejected the evidence but both found more work was needed to understand how to apply the findings in practice. Study A built on these findings and identified areas for further research, including economic analysis and the contribution of temporary staff on outcomes.
Calculating the nursing input The Carter report (Carter 2016) on productivity in English NHS acute hospitals recommended the adoption of Care Hours per Patient Day (CHPPD). This combines the total number of hours worked by both nursing support staff and registered nurses and midwives over a 24-hour period and dividing it by the number of patients in beds at 23:59. NHS Improvement requires that NHS trusts in England report registered nurse hours as a subsection of the overall score.
Other evidence on staffing and care: There is evidence that ward staffing is dynamic and that registered nurse input required varies across the patient’s stay. Study B reported statistical associations between higher numbers of registered nurses in the first week of stroke patients’ admission and increased survival, but the impact was not maintained over later stages of the patients’ inpatient stay. The short-term effect was stronger for registered nurses than support staff, suggesting there is something unique about registered nurse work at this stage of the patient journey. Twigg et al. (2016) evaluated a natural experiment in Australia which introduced an enrolled nurse (a regulated nurse role with a focus on practical nursing skills with a shorter training than registered nurses) into a system without previous experience of such a role. While the registered nurse hours stayed the same, the rate of some adverse events increased. The authors suggest this was due to lower levels of vigilance by registered nurses whose direct contact time with patients was reduced. Both Studies A and B suggest that better understanding of registered nurse work is required with careful consideration given to the relationship between registered nurses and support staff and how the work is divided. This suggests we should be cautious about combining their hours into a single measure of ward staffing provision.
Ward skill mix: Following the registration of nurses in the UK in 1919, the mix of skills in hospital wards has long been a debated area. The Lancet Commission (1932) called for more flexibility leading to the assistant nurse, later known as the state enrolled nurse, in 1943. Many countries have licensed practical nurses but the introduction in the UK of Project 2000 (UKCC 1986) saw the phasing out of the state enrolled nurse. Prior to Project 2000, hospital-employed student nurses had made up a large part of the ward workforce (supported by nursing auxiliaries) and their contribution was replaced by a new, unregulated workforce: the Healthcare Assistant. Educational preparation for unregulated staff varies from a few weeks in-house training to a foundation degree for assistant practitioners. In 2019 a new regulated role, the Nursing Associate will enter the English NHS. This raises the question of what is the most cost-effective mix of skills.
There is some evidence of the impact of support workers on patient outcomes. Jarman et al. (1999) found that higher percentages of A-grade staff (healthcare assistants) per doctor and per bed in English NHS hospitals were associated with higher mortality. However, Study A found the risk of death was higher both when there was an increase in nursing assistant hours compared to the average ward level and also when nursing assistant hours were low, suggesting a more nuanced relationship. Study C found little evidence to suggest that there was any strategic plan about how to use support workers. Senior managers largely considered the role as a substitute for registered nurses and there were multiple different titles and varying complexity and diversity of tasks performed. Whilst registered nurses valued the support roles, they had concerns around the ambiguity of role boundaries.
Our NIHR-funded study (Study C) on support workers fed into the post-Mid Staffordshire and Francis deliberations on the more efficient and effective use of healthcare assistants in acute healthcare settings. More specifically, the study provided the evidence base for the Cavendish Review, which recommended the now widely adopted Care Certificate, a more regulated and standardised approach to the induction of support workers.
Ian Kessler, Professor of Public Policy and Management at King’s College London
Northern Ireland delegation framework
The Nursing and Midwifery Council holds registered nurses accountable for decisions to delegate tasks and duties to support staff. Northern Ireland has developed a framework to help staff make a risk-based decision, taking into account the environment of practice and the professional, legislative and regulatory requirements to underpin effective decisions to delegate. The framework also helps clarify the level of supervision and support required.
http/www.nipec.hscni.net/work-andprojects/adv-guid-info-bt-pract-nurs-mid/deleg-in-nurs-mid/
Study D explored the development and impact of assistant practitioners (higher-level but unregistered support staff with foundation degree preparation) supporting the work of ward-based registered nurses in acute NHS (hospital) trusts in England. The researchers found these roles were mainly driven by external pressures rather than perceived organisational need. Individual organisations were developing roles with little national policy guidance. The consequence was diffuse and confused organisational interpretations of the role. The study found a plethora of different job titles and forms of training for assistant practitioners, which contributed to ongoing confusion about the role. The key discrepancy was the extent to which the role was envisaged as an ‘assistant’.
This need for clarity of roles is likely to extend to the use of volunteers (see below) and the communication with relatives caring for patients. Whilst there is promising evidence about the use of volunteers, some concerns have been raised about how they are used. Fitzsimons et al.’s (2014) evaluation of King’s College Hospital volunteering service found examples where boundaries between professional and volunteer roles were blurred. Ross et al. (2018) recommended hospitals adopt formal volunteering strategies that align volunteering with the organisation’s ways of working.
Evidence on the use of volunteers: The NHS is currently working to increase the scope and opportunities for volunteering in hospitals, including volunteers being directly involved with care. NIHR-funded collaborations in England have been undertaking small feasibility studies with promising findings, although large studies are needed.
Study E surveyed the views of 92 older people over a two month period about the acceptability of the use of volunteers for fundamental care of older inpatients. Most participants thought volunteers could be trained to help with meals and walking. Other tasks identified for volunteers included companionship and talking (19 responses), help tidying the bedside (16 responses), and personal care (12 responses) including washing, escorting to the toilet and cutting nails. Their main reservations were appropriate training and interaction with paid staff members.
Study F trialled the implementation of volunteer mealtime assistants in four different hospital departments (Medicine for Older People, the Acute Medical Unit, Adult Medicine and Trauma & Orthopaedics) and evaluated the practicality of recruiting, training and retaining them on such a large scale. The authors noted that including the volunteers within the ward team was crucial. Patients and ward staff valued the volunteers highly and the volunteering continued after the study finished.
Study G evaluated the feasibility and acceptability of using trained volunteers to increase physical activity of older inpatients. Volunteers encouraged patients to keep active (walk or chair-based exercises) twice a day for about 15 minutes each session. The intervention was well-received by patients and staff. Researchers noted an improvement in physical activity levels, and concluded that it was feasible and safe to train volunteers to mobilise patients. This study has since been adopted by the University Hospital Southampton NHS Foundation Trust as part of its ‘eat, drink, move’ initiative for patients.
Study H looked at the feasibility and acceptability of hospital volunteers to collect patient feedback about the safety of their care. All stakeholders were positive about the intervention and the researchers are continuing to assess the impact on patient safety improvements. A later study (Louch et al. 2018) found that although volunteer led data collection is feasible, using it to effect change was difficult and not all staff viewed it as credible safety information.
Interprofessional working: One of the criticisms of the international literature on ward staffing is the lack of reference to how registered nurses work with other professions based on the same ward. While good multidisciplinary working is widely assumed to be a positive contribution to healthcare, designing a research study to test this has proved challenging. For example, Study I synthesised nine studies that explored whether educational interventions designed to promote interprofessional collaboration improve the quality of care provided and health outcomes, but the authors decided there was insufficient evidence to draw clear conclusions on the effects. Conversely, Study J combined a review of UK and international research evidence and policy with semi-structured interviews and suggests that interprofessional collaboration and coordination of staff was associated with an increase in patient satisfaction and a reduction in length of stay.
Study K investigated the introduction of a new professional role to the UK, the physician associate, to support medical staff in secondary care. Physician associates have a first degree, are trained at postgraduate level in the medical model of care and work under the supervision of a medical practitioner. The study found they undertook much of the ward work for the medical or surgical team. Initial nurse confusion about the role dissipated relatively quickly. The continuity that physician associates provided to the medical and surgical teams as well as their presence on wards meant that nurses reported they helped early escalation of concerns about patients to senior doctors, patient management and overall patient flow.
Study L looked at stroke care pathways. It found that interprofessional teamworking was largely invisible to patients and their carers. Some of the interprofessional teams were very large and this had a number of detrimental effects, including staff feeling too intimidated to contribute; team leaders being less available; team members not knowing each other very well; and ambiguity or conflict over leadership. However, clarity of leadership was found to be highly predictive of overall team performance. The authors concluded that there is a need to consider carefully the size and structure of interprofessional teams in order to strengthen and clarify team leadership.
Are interprofessional pathways simply a series of overlapping teams? Does it matter? The authors of Study L suggest that where there was unambiguous leadership, there was better team performance. However, ambiguity in leadership was a problem identified in this study which, I believe, reflects a wider leadership crisis in healthcare delivery.
Flo Panel-Coates, Chief Nurse, University College London Hospital NHS Foundation Trust
Issues to consider when deciding the shape of the ward team: Determining the size and shape of an inpatient ward team cannot be reduced to a simple algorithm. But despite the limitations, there is a larger body of work showing a relationship between the number of registered nurse hours and safety, effectiveness and patient experience than exists for any other professional staff group. In the absence of perfect information, managers need to make decisions about the shape of the workforce, particularly in challenging economic times. The evidence presented here does not provide a definitive answer. It raises a number of critical questions for decision makers to use when making a risk-based assessment of local need:
- Do new roles change the nature of registered nurse work? Do they divert them from the direct contact and vigilance of patients that the evidence shows is critical for safety?
- Does increased input from other clinical professionals affect the amount of registered nurse hours required?
- How are unregistered workers used? Are they complementing the professions or substituting for them?
- Is there clarity within the team about the different roles, who does what and who is accountable for what? Are there clear delegation frameworks?
- Are there clear and effective systems for handing over information and following up delegated tasks?
Managing the team and the ward
Clinical productivity, or getting the best clinical outcomes for the resources provided, appears to be closely aligned with the way in which staff work together. Lalfond and Charlesworth (2017) found that hospital consultant productivity fell between 2009/10 and 2015/16 at a time of rapidly rising consultant numbers. Analysis indicated that 56% of the variation in consultant productivity at the hospital level could be explained by a number of factors, including the number of registered nurses and clinical support staff within the hospital workforce. This suggests that looking at the productivity of one professional group in isolation is unhelpful.
In addition, Dixon et al. (2018) suggest that large gains in clinical productivity can be made from good management, ensuring staff welfare and training in quality improvement methods.
Staff retention and wellbeing: Retaining staff is key, and in particular retaining experienced staff. Halter et al.’s two (2017a and 2017b) systematic reviews on the causes of nursing turnover found moderate quality evidence that nurse stress and dissatisfaction were the most significant personal issues. Managerial and supervisory behaviours were the most important organisational factors. They found the research evidence on interventions to reduce turnover was generally weak but there was some evidence that preceptorship (additional support for newly qualified staff) and good ward leadership that enhances group cohesion can decrease turnover and increase retention of nurses.
Nurses want to work in positive environments. The survey of English nurses for the RN4Cast study (Ball et al. 2012) found the strongest associations with overall satisfaction in current jobs were professional status, independence at work and opportunities for advancement.
Satisfaction and intention to stay are associated with flexible approaches to how ward staff are deployed. Study M is a systematic review of the effect of hospital nurse staffing models on patient and/or staff-related outcomes. It reported that some management systems improve staff-related outcomes, particularly primary nursing (where each patient has a named nurse to manage their care plan) and self-scheduling. However, they advise caution due to the limited evidence available. Kitson et al. (2013), in their evidence synthesis, found that a positive practice environment (based on values, professional relationships and the patient care delivery model) improved recruitment and retention. Hayward et al. (2016) reported that Canadian nurses’ decisions to leave were influenced by poor relationships with physicians and poor leadership, leaving them feeling ill-equipped to perform their job. Similar findings were observed in Italy by Galetta et al. (2013) and across 10 European countries (Heinen et al. 2013). This reflects the work of the American Nurses Credentialing Centre’s ‘Magnet’ Recognition Program. Based on work that started in 1983 identifying the 14 forces that act as a magnet to attract and retain nurses in US hospitals, this high profile accreditation system reflects the wider literature on psychology at work. However Petit and Regnaux’s (2015) systematic review of performance and quality in these hospitals found mixed results with varied research quality and could not conclude that obtaining Magnet accreditation has a causal effect on either nurse or patient outcomes.
Study N found staff morale was associated with good teamworking and amongst other findings, the researchers reported that job design factors have high influence on staff morale. While high job demands are associated with psychological strain, having a large amount of control over how the job is done can mitigate this, together with support from peers and managers. Although undertaken in mental health settings rather than acute hospitals, the findings around role definition (role clarity), fairness and communication within the team are consistent with other studies in this review.
Our research suggests that fundamental to healthcare is professionals working together to a high standard of teamwork. They must have clear, shared objectives aligned with providing high quality and compassionate care; clear roles; regular and engaging team/ward meetings; a commitment to nurture positive, supportive, compassionate relationships with each other and their patients; they must quickly work through conflict, preventing intense or chronic conflicts; value diversity; lead inter-team cooperation and, regularly take time out to review their performance and functioning and how to improve. It is not only about staffing levels but about how we work together.
Michael West, Professor of Work and Organisational Psychology, Lancaster University Management School
Good leadership and support for staff was also found to be important in Study O. This systematic review reported that staff wellbeing is linked to staff engagement and conversely a lack of engagement is associated with burnout. Job satisfaction and perceived control over own work are more likely to lead to high levels of staff engagement and there was some evidence that a highly engaged team increases the engagement of individual members. However, the authors caution that only a small proportion of studies in the review were based in healthcare settings.
The importance of local (ward) leadership and climate was also highlighted in Study P, together with the importance of education and development for staff in local leadership roles.
The importance of emotional reserves in maintaining staff wellbeing and ultimately in staff retention has led to interest in interventions to reduce emotional exhaustion. Study Q evaluated the introduction of Schwartz Rounds in the NHS. Schwartz Rounds are monthly group meetings open to all staff in healthcare organisations, where staff discuss the emotional, social and ethical challenges of care in a safe environment. Psychological health improved in staff who attended Schwartz Rounds but not in those who did not attend. Reported outcomes included reduced isolation; improved teamwork and communication; and reported changes in practice. Findings suggest Schwartz Rounds are a ‘slow intervention’ that develop their impact over time.
Featured study
Patient experience improves when staff wellbeing is high Whilst many factors influence high quality patient care, staff wellbeing was shown to be an antecedent of good patient care delivery. Patients noticed this and witnessed that staff demeanour and behaviour was linked to workplace conditions including workload, the physical environment and the way staff are managed and led. Six factors or ‘bundles’ were found to influence staff wellbeing: local (team) work climate (described by some staff participants as contributing to feelings of ‘family at work’); co-worker support, job satisfaction, perceived organisational support, low emotional exhaustion and supervisor support. Interdependencies between these different aspects of staff wellbeing meant that no single factor could be identified as the key. However, local climate was much more strongly associated with good care than organisational climate, highlighting the importance of the local work climate – peers and team and the immediate supervisor (such as ward manager) role.
Schwartz Rounds are a multidisciplinary forum designed for staff to come together once a month to discuss and reflect on the nonclinical aspects of caring for patients - that is, the emotional and social challenges associated with their jobs. Schwartz Rounds (developed by The Schwartz Center for Compassionate Care in Boston, US) are designed to foster relationships, enhance communication, provide support and improve the connections between patients and caregivers. Attending Rounds can be experienced as both supportive and transformative and staff attending Rounds report (Lown & Manning, 2010) (Goodrich, 2012):
- Decreased feelings of stress and isolation »» improved team work and interdisciplinary communication
- Increased insight into social and emotional aspects of patient care and confidence to deal with non-clinical issues relating to patients
- Changes in departmental or organisation wide practices as a result of insights that have arisen from discussions in Round
I really appreciated the language. You hear words used you don’t normally hear such as anger, guilt, shame and frustration. They are obviously there, but there is no outlet for them.
Staff participant – Schwartz Round: courtesy of the Point of Care Foundation
Case study: retaining nurses at Yeovil District Hospital
NHS Improvement in partnership with NHS Employers launched a retention programme in England in June 2017 giving trusts the tools, knowledge and expertise to develop initiatives that will encourage staff to stay working for the NHS. Yeovil District Hospital NHS Foundation Trust formed part of cohort one of the retention programme. Between June 2017 - June 2018, the trust reduced its nursing staff turnover rate by 3.3% by focussing on a number of key areas:
- Culture and leadership
- Health and wellbeing
- Personal and career development
Managing staff Decisions about the number of staff and the mix of skills use a combination of top down (e.g. benchmarking against other hospitals) and bottom up (e.g. modelling) approaches. These are often mediated by professional judgement. The demand for staff on a day-to-day basis can be highly variable. Hospitals are seeing increasing spend on unscheduled enhanced care, or ‘specialling’ (one-to-one care to ensure the safety of patients who may be suffering from cognitive impairment, exhibit challenging behaviour, or may be at risk of falls or of causing harm to themselves or others). Wood et al. (2018) reviewed the evidence and concluded there is a wide variation in what one-to-one care entails. Enhanced care is rarely mentioned when planning ward staffing requirements.
Whilst NICE endorses some resources to assist decision makers, they note that there is little evidence for the costs effectiveness of using any tool. Many of the tools are based on patient acuity rather than nursing workload (these two are not synonymous). An ongoing study (Study R) is currently evaluating one of the tools endorsed by NICE, the Safer Nursing Care Tool.
Study S explored how NHS managers use workforce management tools and technologies to determine staffing in individual hospitals. Using a variety of data sources, the researchers developed a realist program theory (a theory driven logic model with propositions that are then tested in practice). They conclude that the way tools are used is dependent on the level of commitment from leaders at all levels of the organisation. Managers need training to use these tools well and to develop their professional judgement. The researchers suggest leadership and communication skills are needed to manage the challenges resulting from the decisions they reach about staffing.
Managing the daily nurse staffing requirements within a large acute trust is incredibly challenging, with the daily reality very different to the theory used when setting establishments and skill mixes. The fast pace of an acute setting results in changing acuity over the course of the day, with the prime focus being to maintain patient safety and ensuring the right staff are available to deliver quality, therapeutic patient care. These needs have to be balanced against financial challenges and using temporary resource efficiently.
Nicky Sinden, Lead Nurse for Workforce, Portsmouth Hospitals NHS Trust
Managers also need skills to deal effectively with sickness and absences. Study T is a small study that trialled an e-learning health promotion intervention for managers to help improve employee wellbeing and reduce sickness absence. It reported managers had insufficient time to engage with the training (highlighting the need to provide ward and unit leaders with dedicated time for managing team wellbeing) and lack of senior management ‘buy-in’. In total, 21 managers used the e-learning tool, completing at least three of the six modules but wellbeing scores for staff showed little difference from the control group. The researchers concluded that the training needed to be better integrated with organisational processes and everyday practice for it to be effective.
Organising care on the wards
Staff who are engaged and enjoying their jobs also need environments where the work is effectively organised. There are many initiatives to change the way staff work. Whilst some are well evidenced, others are developed without supporting evidence and high quality evaluation. What emerges from the literature is that national initiatives are defined and implemented in highly variable ways, making evaluation of their impact challenging.
One area that has received attention is interruptions. Westbrook et al. (2017) note a steady increase in the number of studies reporting interventions designed to reduce interruptions to nurses during the preparation and administration of medications. Their study of a ‘Do not interrupt’ bundled intervention (wearing a coloured tabard when administering medications; strategies for diverting interruptions; clinician and patient education) showed the intervention was most effective at reducing interruptions from other nurses. The intervention had no substantial impact on the rate at which patients interrupted the nurse. Nurses reported a number of practical issues, including the difficulty of taking vests on and off, and concerns that medication administration took longer.
Similarly schemes to protect mealtimes (intuitively a good thing) are widely promoted. However, Porter et al.’s (2017) systematic review concluded that, given the small number of observational studies and the quality of evidence on the effect of the intervention on nutritional intake, there is insufficient evidence for widespread implementation of protected mealtimes in hospital.
The way in which the work is organised also has an impact on the efficiency of the team and staff morale.
A major initiative to improve the way in which ward care is organised (Productive Ward) was developed in 2005 by the NHS Institute for Innovation and Improvement. Study U is a ten year evaluation of its impact and sustainability. The findings suggest that tools can be useful but that sustainable improvement at ward level will require additional input, including educating ward staff of all levels in the underlying principles of Lean working, and refreshing training and activities as staff and contexts change.
Featured Study U
Little quantitative evidence of sustained impact over time from Productive Ward initiative: Study U evaluated the 10-year impact of an improvement programme in English NHS trusts. Productive Ward is a quality improvement intervention developed to provide tools to engage frontline staff in the implementation of change at ward level. Based on Lean management principles, a number of modules were developed to: (1) increase time nurses spend in direct patient care, (2) improve experience for staff and patients, and (3) make structural changes on wards to improve efficiency.
A report commissioned by the NHS predicted a £270 million benefit would be yielded from implementing Productive Ward across 139 acute trusts in NHS England by March 2014. The researchers demonstrated that against this backdrop there was there was strong normative pressure on Directors of Nursing to adopt Productive Ward.
Following early adoption by a large proportion of acute hospitals in England, none did so after 2012. Adherence to the recommended approach to implementation was highly variable. The average length of use of Productive Ward was three years and a majority of Directors of Nursing surveyed said that the programme is no longer being implemented in their organisation. When the researchers conducted their fieldwork in 2017- 18, changes made to ward layouts and to specific ward processes remained evident and these were credited by study participants with improving staff and patient experience (largely through releasing time). However, there is little quantitative evidence of impact over time or whether initial improvements were sustained.
Another high profile initiative has been Intentional rounding: structured registered nurse ward rounds to address concerns about quality of care on the wards. Study V reviewed the literature, drawing on the process developed in the US whereby nurses carry out one to two hourly checks with every patient using a standardised protocol and documentation. The review highlights the ambiguity surrounding its purpose and limited evidence of how it works in practice. The researchers highlight that without good preparation and understanding of its purpose, there is potential to increase the frequency of nurse–patient communication, but not necessarily to improve its quality. Further NIHR work to evaluate practice in the UK is ongoing.
Issues to consider when managing the team on the ward: Staff morale has a direct influence over patient experience of care as well as on retention of staff. Staff morale, and staff engagement, are influenced by a range of factors including management behaviours and the ward climate. Ward climate is the shared understanding of ‘how things are done around here’ and influences the effectiveness and efficiency of specific aspects of work. There is an advantage to standardising ward processes and ensuring all ward staff have clarity of what is expected of them, but these need to be integral to the way the team work rather than bolted on. Managers and senior nurses considering how to improve the management of ward work and of the team should consider the following:
- Do we understand the ward climate and how new work processes might affect it?
- Do we link data on patient experience and outcomes to ward climate and leadership?
- What are the goals of new process and how will we know whether they have been realised?
- Do we ensure ward staff fully understand improvement techniques?
- Is the anticipated improvement worth the effort? Could the effort involved be used elsewhere with a larger gain?

Gaps in the evidence
This report is, at best, a partial review of the evidence. We know more about nurse staffing on general acute wards than we do about many other staff groups and settings, but there are still many uncertainties. Research on workforce has received relatively little funding and support in the past. This is changing and our review shows some areas where the NIHR and other research has given us good insights and understanding of the everyday challenges facing managers, staff and patients on the ward.
While we have not carried out a systematic exercise to identify gaps in evidence, there are some obvious areas where more work could be done. The research has largely focused on the link between registered nurses and a range of adverse events. Work has begun on understanding the nature of that relationship and more research is needed on the contribution of ward staff to positive outcomes and clinical effectiveness.
NICE (2014) identified the lack of economic evaluations to assess the relative value of different kinds of staff input. Whilst evidence is beginning to emerge, more studies are needed.
Most of the evidence fails to consider the contribution of other health professionals. There is a need for evidence that considers models with different levels of other healthcare professionals’ hours at ward level. The role of temporary and agency staff on the ward is also under-examined.
The role of support workers needs further exploration, including their educational preparation and supervision. Evidence is needed on where the boundaries with registered nurse work should be drawn, together with ways of supporting delegation and the flow and transfer of information relevant to patient care across the ward team.
The ward environment is changing, with the introduction of electronic records and electronic patient monitoring. A better understanding of the implications for ward staffing and workflow of new digital technology is required.
As the hospital population continues to age, with greater acuity and prevalence of other conditions such as dementia, the increasing contribution of relatives (as currently seen in paediatric wards) and the use of volunteers are both significant changes that may have material effect on the shape and work of the ward staff. Research into the risks and benefits will be needed.
Conclusion
The evidence demonstrates that making decisions about ward staffing is complex. We know that there is a relationship between the level of nurse staffing and patient outcomes, but we do not know exactly what is a safe level or the optimal skill mix of a team for individual wards. Determining the right number of staff and mix of education and skills is not a precise science and requires a risk assessment based on the best available evidence. Measuring the impact of staffing on outcomes requires robust measures that reflect the complexity. This includes further work “to develop metrics and systems that reflect wider structural factors that underpin nursing quality such as staffing, skills mix and staff experiences and link to other quality care metrics such as patient experience” (Maben et al. 2012).
There are a number of different decisions to be made about ward staffing. Firstly, the decision about the planned numbers of workers for each ward is a pragmatic decision. Decisions are based on a combination of the evidence, professional judgement and available resources (money and people). The evidence presented in this review can help to assist in the assessment of the risks associated with different staffing configurations. People making these decisions need education and training and provider organisation boards should articulate the levels of risk that they can tolerate.
Planned staffing must be matched with local decisions around fluctuating case mix and workload together with day-to-day absences in the planned staffing. The evidence shows that there are aspects of the workload which may be better undertaken by registered nurses in order to prevent avoidable patient harms, including close, direct observation of patients. Consideration of ward staffing should therefore separate registered nurse hours from assistant and support workers. The different scope of work of registered nurses, assistant practitioners and support staff together with other members of the wider team need to be clearly defined. The evidence suggests that calculations of registered nurse hours required should include sufficient time to supervise support workers. Close attention should be paid to the impact of the new nursing associate role, in particular its impact on the work of registered nurses.
Determining the makeup of the workforce is only part of the picture. Whilst there is clearly a threshold of unsafe workload, the evidence demonstrates that the way staff are managed and the work processes contribute to the staff’s capacity to provide safe and effective care. Moreover, management and ward processes have been shown to significantly influence the retention of staff. Efficient ward processes can reduce duplication and enhance staff morale, although care should be taken to avoid top down processes that conflict with local practices or increase work at ward level. The role of the ward manager has been shown to be pivotal in creating the highest levels of staff wellbeing and engagement; two factors that are key determinants of available hours on a dayto- day basis. There are a number of interventions that can help the ward manager to achieve this, from creating a positive practice environment to Schwartz Rounds as well as the management of individual staff.
It is clear that good local, real time intelligence is needed to respond to fluctuating need. The complex relationship between ward staffing and outcomes mean that there are no simple indicators that measure the impact of different staffing models. There has been research that informs decisions but its application requires managers and senior nurses with good understanding of the evidence. More work is needed to develop assurance frameworks that can encapsulate this complexity and to ensure high quality data is collected to populate them and to form the basis of future research studies.
Finally, getting the most out of staff requires good leadership to create positive ward environments and to support individual members of staff. Ward leadership shapes how staff are deployed, sets standards for staff to follow, and is key to creating a safe and healthy climate for both staff and patients. Investment in developing the skills of ward leaders to do this and ensuring they have protected time to deliver has been shown to be key in providing high quality care as well as attracting and retaining staff.
My own ward observations support the findings in the report regarding the importance of high quality leadership within wards and the value of a systematic, team environment.
Ron Capes, Lead Governor, Basildon and Thurrock University Hospitals NHS Foundation Trust
Study summaries
STUDY A (HS&DR 13/114/17)PUBLISHED
Published, 2018, Principal Investigator Griffiths P
This study examined how registered nurse and healthcare assistant staffing levels relate to missed or delayed observations of vital signs (including patients’ blood pressure, pulse and breathing) and to death in hospital, adverse event (death, cardiac arrest or unplanned intensive care admission) and length of stay. It looked at data routinely collected by 32 general adult wards of an acute NHS hospital on staffing levels and electronically recorded patient observations and outcomes, involving 138,133 admissions from 2012 to 2015. Researchers found that higher registered nurse staffing levels were associated with fewer missed observations, reduced length of stay and less adverse events, including mortality. Patients who spent time on wards with fewer than the usual number of registered nurses were more likely to die, or to stay in hospital for longer. The relationship between registered nurse staffing levels and patient mortality appeared to be linear. By contrast, the effect of healthcare assistant levels was less clear, with the hazard of death increasing when patients experienced either above- or below-average healthcare assistant staffing. Although missed observations explained some of the links between nurse staffing levels and hospital death rates, there are other causal pathways so these records cannot guide staffing decisions. The authors noted that healthcare assistants are unlikely to make up for a shortfall of qualified nurses. More evidence is required to confirm approaches to setting staffing levels.
Griffiths P, Maruotti A, Recio Saucedo A, Redfern OC, Ball JE, Briggs J et al. Nurse staffing, nursing assistants and hospital mortality: retrospective longitudinal cohort study. BMJ Quality & Safety 2018. Published Online First: 04 December 2018.
http://dx.doi.org/10.1136/bmjqs-2018-008043
Griffiths P, Ball J, Bloor K, Böhning D, Briggs J, Dall’Ora C, et al. Nurse staffing levels, missed vital signs and mortality in hospitals: retrospective longitudinal observational study. Health Serv Deliv Res 2018;6(38)
https://doi.org/10.3310/hsdr06380
STUDY B (HS&DR 12/128/48) PUBLISHED
Published, 2017, Principal Investigator Doran T
This study explored the higher risk of death of people admitted to hospital during out-of-hours periods. Researchers looked at emergency admissions data for all 140 non-specialist acute hospital trusts in England between April 2013 and February 2014 (n=over 12 million accident and emergency attendances and 4.5 million emergency admissions). They also analysed emergency admissions between April 2004 and March 2014 for one large acute NHS trust (n=240,000 admissions). They compared deaths within 30 days of attendance or admission for normal working hours and out-of-hours periods (weekends and nights). Nationally, after taking account of how sick patients were, the risk of death was no higher for patients admitted outside normal working hours, with the exception of Sunday daytimes. In one acute stroke unit, having more, and registered, nurses present during the first hours of admission was associated with increased patient survival in the first week, but not over longer periods. The researchers concluded that it is likely to be more cost-effective to extend services for key specialities over critical periods than to implement seven-day services. Future research could identify these key specialities and times.
Han L, Meacock R, Anselmi L, Kristensen SR, Sutton M, Doran T, et al. Variations in mortality across the week following emergency admission to hospital: linked retrospective observational analyses of hospital episode data in England, 2004/5 to 2013/14. Health Serv Deliv Res 2017;5(30)
https://doi.org/10.3310/hsdr05300
STUDY C (HS&DR 08/1619/155) PUBLISHED
Nature and consequences of support workers in a hospital setting
Published, 2010, Principal Investigator Kessler I
This three-year study examined the role of support workers in hospitals, particularly healthcare assistants. Senior staff were interviewed in nine NHS trusts in the south, midlands and north. Case studies of four trusts (one in each region and London) involved interviews with healthcare assistants, registered nurses and managers (n=273), observations of healthcare assistants, ward housekeepers and registered nurses (n=275 hours) and focus groups with former patients (n=94). Surveys in each trust included healthcare assistants (n=746), registered nurses (n=689) and former patients (n=1651). Findings indicated that senior managers considered healthcare assistants partly as a substitute to achieve cost efficiencies, but also as a way of relieving registered nurses of certain routine tasks. Healthcare assistants’ roles varied, with differences between trusts. Most commonly, they delivered routine technical tasks, traditionally the preserve of registered nurses. Some healthcare assistants had extended their role significantly, but were often paid at Band 2 rather than 3. Healthcare assistants were generally satisfied with their jobs. Many aspired to be nurses, but trusts did not tend to address this. Registered nurses valued healthcare assistants, although they sometimes had concerns about the delegation of tasks to them, and their accountability for them. Patients could often relate to healthcare assistants more easily than to registered nurses. Patients could not easily distinguish healthcare assistants from registered nurses but, when they could, their care experience was more likely to be positive.
Kessler I, Heron P, Dopson S, Magee H, Swain D. Nature and Consequences of Support Workers in a Hospital Setting. Final report. NIHR Service Delivery and Organisation programme; 2010.
https://www.journalslibrary.nihr.ac.uk/programmes/hsdr/081619155/#/
STUDY D (HS&DR 08/1619/159) PUBLISHED
Published, 2010, Principal Investigator Spilsbury K
This mixed methods study investigated the role of assistant practitioners in acute NHS Trusts in England. Assistant practitioners are workers who have undertaken a formal qualification, for example a national vocational qualification or foundation degree. Researchers undertook case studies at three trusts, involving 13 wards. Data collection included analysis of assistant practitioner job descriptions (n=22), observations of staff activity (n=15,355) and interactions with patients (n=17,543), questionnaires (270 returned, response rate 52%), interviews (n=105) and focus groups (n=31 participants) with registered nurses, assistant practitioners and healthcare assistants. A national survey of 40 acute trusts (381 responses overall, response rate 35%), and a literature review, added context. Results indicated that organisations were developing assistant practitioner roles with little national policy guidance. Confusion about whether assistant practitioners were ‘assistants’ or ‘substitutes’ for registered nurses was compounded by inconsistency in job titles, training and pay bands. Assistant practitioners’ responsibilities fluctuated. Registered nurses were reluctant to delegate tasks due to concerns about accountability. Assistant practitioners were generally valued for contributing to patient care, providing leadership to healthcare assistants, and supporting new nurses. Opportunities for career progression seemed limited. Assistant practitioners felt that registration and regulation were important for future development of the role. Further research could evaluate the role in varying contexts, its impact on patient outcomes and its cost-effectiveness.
Spilsbury K, Adamson J, Atkin K, Bartlett C, Bloor K, Borglin G et al. Evaluation of the Development and Impact of Assistant Practitioners Supporting the Work of Ward-Based Registered Nurses in Acute NHS (Hospital) Trusts in England. Final report. NIHR Service Delivery and Organisation programme; 2010.
https://www.journalslibrary.nihr.ac.uk/programmes/hsdr/081619159/#/
STUDY E (CLAHRC WESSEX) PUBLISHED
Acceptability of use of volunteers for fundamental care of older inpatients
Published, 2015, Principal Investigator Baczynska AM
This study explored the views of older people about the involvement of volunteers and family in the delivery of fundamental care in hospital. Ninety-two older people (aged 60-99 years, 74% female) were surveyed at lunch clubs (n=32 clients and 10 volunteers), a nursing home (n=11 residents) and acute medical wards in a hospital (n=38 in-patients and one relative). Forty-one respondents had experience of hospital volunteers and rated this highly. Most thought volunteers, with appropriate training, could help with meals and walking. Other tasks that some thought suitable for volunteers were: companionship and talking (n=19), tidying the bedside (n=16), and personal care (n=12) including washing, escorting to the toilet and cutting nails. Reservations included appropriate training, potential clashes with paid staff, and overcrowding on the wards. Over half of respondents would choose to regularly help paid staff in caring for a relative in hospital. Overall, the concept of volunteers and family members contributing to fundamental care in hospital was acceptable to the respondents.
Baczynska AM, Blogg H, Haskins M, Aihie Sayer A, Roberts HC. Acceptability of use of volunteers for fundamental care of older inpatients. Age and Ageing 2015 Apr; 44(suppl_1): i1.
https://doi.org/10.1093/ageing/afv029.01
STUDY F (CLAHRC WESSEX) PUBLISHED
Published, 2014, Principal Investigator Roberts HC
This study investigated the feasibility and acceptability of volunteers assisting older patients on an acute female medical ward with weekday lunches, over one year (February 2011 to January 2012). A volunteer training programme was developed and researchers conducted interviews and focus groups with volunteers (n=12), patients (n=9) and nursing and support staff (n=17). Of 59 potential volunteers, 38 attended a training session developed by the hospital speech and language therapist and dietitian. Volunteers were observed providing mealtime assistance, and their competency was assessed against set criteria. Twenty-nine volunteers went on to deliver mealtime assistance, including feeding, and 17 were still volunteering at the end of the year. In all, 3911 patients received assistance over the year. The authors noted that including the volunteers within the ward team was crucial. The volunteers were positive about their training and ongoing support. Patients and ward staff valued the volunteers highly. A subsequent study, from August 2014-December 2015, evaluated the wider implementation of the mealtime assistance programme in nine wards in one hospital (across Medicine for Older People, Acute Medical Unit, Trauma and Orthopaedics and Adult Medicine departments). Volunteers were trained to help patients aged 70 or over at weekday lunchtime and evening meals. Sixty-five volunteers helped at 846 meals over 15 months. A researcher interviewed patients (n=8) and staff (n=7), and conducted a focus group with volunteers (n=9). Patients and nurses universally valued the volunteers, who were skilled at encouraging reluctant eaters. Volunteers, patients and staff all saw training as essential. Cost analysis suggested that the programme released valuable clinical time. Limitations included the study being single-site.
Roberts HC, De Wet S, Porter K, Rood G, Diaper N, Robison J et al. The feasibility and acceptability of training volunteer mealtime assistants to help older acute hospital inpatients: the Southampton Mealtime Assistance Study. Journal of Clinical Nursing 2014; 23(21-22):3240-9.
https://doi.org/10.1111/jocn.12573
Howson FFA, Robinson SM, Lin SX, Orlando R, Cooper C, Sayer AA, Roberts HC. Can trained volunteers improve the mealtime care of older hospital patients? An implementation study in one English hospital. BMJ Open 2018;8:e022285. doi:10.1136/bmjopen-2018-022285.
https://bmjopen.bmj.com/content/8/8/e022285
STUDY G (CLAHRC WESSEX) COMPLETED, INTERIM PUBLICATIONS
Interim publications, 2018, Principal Investigator Roberts HC
This study evaluated the feasibility and acceptability of using trained volunteers to increase the physical activity of older people in hospital. Low mobility of older people in hospital is associated with poor health outcomes. Volunteers were trained to encourage older inpatients to keep active for two 15 minutes sessions per day. Activity involved walking or chair based exercises. Outcomes measured were patient activity levels, cognition, mood and quality of life. Seventeen volunteers were recruited, and 12 retained (71% retention). 310 sessions were offered, of which 230 were delivered (74% adherence). The intervention was well-received by patients and staff. Researchers noted an improvement in physical activity levels, and concluded that it was feasible and safe to train volunteers to mobilise patients. This programme, together with the mealtime assistance programme, has since been adopted by the University Hospital Southampton NHS Foundation Trust as part of its ‘eat, drink, move’ initiative for patients. From autumn 2017, volunteer mealtime and mobility assistants have been embedded in clinical services and teams, and trained and supported by University Hospital Southampton staff. Future work may include a multicentre controlled trial.
Lim SER, Dodds R, Bacon D, Sayer AA, Roberts HC. Physical activity among hospitalised older people: insights from upper and lower limb accelerometry. Aging Clin Exp Res 2018; 30(11): 1363–1369. Published online 2018 Mar 14.
https://dx.doi.org/10.1007%2Fs40520-018-0930-0
https://www.clahrc-wessex.nihr.ac.uk/theme/project/36
STUDY H (CLAHRC YORKSHIRE & HUMBER) PUBLISHED
Published, 2017, Principal Investigator O’Hara J
This study explored the feasibility and acceptability of hospital volunteers collecting patient feedback about the safety of their care, using the Patient Reporting and Action for a Safe Environment (PRASE) Intervention. The intervention involves a facilitated discussion at the patient’s bedside, and was previously explored in a randomised controlled trial. The pilot phase of the study, involving two acute NHS trusts from July 2014-November 2015, comprised five focus groups with hospital volunteers (n=15), and interviews with voluntary services and patient experience staff (n=3) and ward staff (n=4). All stakeholders were positive about the intervention, and the use of volunteers. Volunteers identified the need for appropriate training and support, while staff concentrated on the necessary infrastructure for implementation, and raised concerns about sustainability in practice. This pilot did not collect patient views. These findings informed the roll-out of the PRASE intervention to multiple wards across three NHS trusts. Researchers will evaluate this roll-out and whether the patient feedback collected by volunteers led to patient safety improvements. Louch G, O’Hara J, Mohammed MA. A qualitative formative evaluation of a patient-centred patient safety intervention delivered in collaboration with hospital volunteers. Health Expectations 2017;20(5):1143-1153.
https://doi.org/10.1111/hex.12560
STUDY I (COCHRANE EFFECTIVE PRACTICE AND ORGANISATION OF CARE GROUP) PUBLISHED
Interprofessional education: effects on professional practice and healthcare outcomes
Published, 2013, Principal Investigator Reeves S, Corresponding author Zwarenstein M
This updated systematic review added nine new studies to the six studies from a previous update in 2008. The 15 studies comprised eight randomised controlled trials, five controlled before and after studies, and two interrupted time series studies. The authors graded the quality of the evidence low to very low. All the studies measured the effectiveness of interprofessional education interventions, where members of different social and/or health care professions learn together, interactively, with the aim of improving collaboration or patient health, or both. These interventions were compared to no educational intervention. Seven studies reported positive outcomes for healthcare processes or patient outcomes, or both, four studies reported mixed outcomes (positive and neutral) and four reported no effects. The authors noted that the small number of studies, their varying design and outcome measures, and the fact that none of them compared interprofessional with profession-specific education interventions, meant that they could not draw clear conclusions about the effects of interprofessional interventions. The evidence base has grown, but further research is needed to address these gaps.
Reeves S, Perrier L, Goldman J, Freeth D, Zwarenstein M. Interprofessional education: effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev 2013; 3:CD002213.
https://doi.org/10.1002/14651858.CD002213.pub3
STUDY J (HS&DR - 08/1319/050) PUBLISHED
Workforce and health outcomes - scoping exercise
Published, 2004, Principal Investigator Sheldon T
This scoping study comprised a review of research evidence and policy (including from outside the UK), and 19 semistructured interviews with heads of UK health-related organisations. It assessed evidence about the impact of different mixes of medical and nursing staff on quality, clinical effectiveness, health outcomes and length of hospital stay. The policy documents and interviews suggested that the NHS, at that time, was making staffing decisions based on activity, rather than outcomes. Most of the included studies reported that better health outcomes were associated with higher doctor:patient and/or nurse:patient ratios, but the study methods had some weaknesses. Most studies suggested that patient outcomes changed little in some areas where nurses substituted for doctors, but these studies were limited in scope. Length of stay and patient satisfaction tended to improve with greater staff collaboration. Evidence on skill mix and wellbeing was limited. Overall, the variations in the methods of the studies, and poor quality evidence in some areas, made combining their results and drawing firm conclusions difficult. The authors concluded that more comprehensive research was needed to evaluate the relationship between staffing levels, skill mix and outcomes.
Hewitt C, Lankshear A, Kazanjian A, Maynard A, Sheldon T and Smith K. Health Service Workforce and Health Outcomes: A Scoping Study. Report for the National Coordinating Centre for NHS Service Delivery and Organisation.
https://www.journalslibrary.nihr.ac.uk/programmes/hsdr/081319050/#/documentation
STUDY K (HS&DR 14/19/26) COMPLETED, WAITING TO PUBLISH, INTERIM PUBLICATIONS
Interim publications, 2018-2019, Principal Investigator Drennan VM This mixed methods study investigated the physician associates contribution to hospital medical teams. Physical associates are trained, following entry with a first degree (usually in biomedical science), at a post-graduate level in the medical model to undertake medical histories, physical examinations, investigations, diagnosis and treatment within their scope of practice as agreed with their supervising doctor. At the time of the study physician associates were not a regulated profession although this will change soon. This multi-phase study included: a systematic review, policy review, national surveys of medical directors and physician associates, case studies within six hospitals utilising physician associates in England and a pragmatic retrospective record review of patients in the emergency department attended by physician associates and foundation year two doctors. The surveys found a small but growing number of hospitals employed physician associates. From the case study element it was found that medical and surgical teams mainly used physician associates to provide continuity to the inpatient wards. Their continuous presence contributed to: smoothing patient flow, accessibility for patients and nurses in communicating with the doctors and releasing doctors’ (of all grades) time for more complex patients and attending patients in clinic and theatre settings and patient safety. Physician associates undertook significant amounts of ward-based clinical administration related to the patients’ care. The lack of authority to prescribe or order ionising radiation (as a non-regulated profession) restricted the extent physician associates assisted with the doctors’ workload. This study was unable to quantify the impact on service delivery or patient outcomes of one, relatively new and small, professional group within complex multi-team acute care systems and service delivery. Physician associates can provide a flexible advanced clinical practitioner addition to the secondary care without drawing from existing professions such as nurses.
Halter M, Wheeler C, Pelone F, Gage H, de Lusignan S, Parle J et al. Contribution of physician assistants/associates to secondary care: a systematic review. BMJ Open 2018;8:e019573
http://dx.doi.org/10.1136/bmjopen-2017-019573
Drennan VM, Halter M, Wheeler C, Nice L, Brearley S, Ennis J et al. What is the contribution of physician associates in hospital care in England? A mixed methods, multiple case study. BMJ Open. 2019 Jan 30;9(1):e027012.
http://dx.doi.org/10.1136/bmjopen-2018-027012
https://www.journalslibrary.nihr.ac.uk/programmes/hsdr/141926#/
STUDY L (HS&DR 08/1819/219) PUBLISHED
Interprofessional team-work across stroke care pathways: outcomes and patient and carer experience
Published, 2013, Principal Investigator Harris R
This mixed methods study examined interprofessional team working across the stroke care pathway. Evidence suggested that stroke patients cared for by interprofessional teams had better outcomes. Existing literature was analysed and research conducted with five stroke teams: two acute, one inpatient rehabilitation and two community teams. Researchers initially interviewed senior staff (n=19). They interviewed patients (n=50) and carers (n=33) two or three times along their care pathway, and staff (n=56) across the five teams. They surveyed all team members (n=263) about team characteristics (response rate=69%) and quality of life at work (response rate=56%), and observed team meetings. The study concluded that patients and carers do not necessarily notice interprofessional working despite its importance in their care; communication with staff is what they value highly. Staff noticed team working far more. Large teams made it harder for everyone to get involved, and had more conflict over leadership. Clear leadership was strongly associated with staff perceptions of better team performance, which in turn was associated with work related quality of life. Nursing staff seemed least involved in the interprofessional team despite having the most contact with patients and carers. Performance targets for single professional groups were a disincentive to collaborative working.
Harris R, Sims S, Hewitt G, Joy M, Brearley S, Cloud G et al. Interprofessional teamwork across stroke care pathways: outcomes and patient and carer experience. Final report. NIHR Service Delivery and Organisation programme; 2013.
https://www.journalslibrary.nihr.ac.uk/programmes/hsdr/081819219
STUDY M (COCHRANE EFFECTIVE PRACTICE AND ORGANISATION OF CARE GROUP) PUBLISHED
Hospital nurse staffing models and patient and staff-related outcomes
Published, 2011, Principal Investigator Butler M
This systematic review included 15 studies about the effect of hospital nurse staffing models on patient and/or staffrelated outcomes. The studies were conducted in the UK, Netherlands, United States, Canada and Australia, published from 1977-2007. The quality of evidence overall was very limited. Many studies judged to have an inadequate design were excluded. The 15 included studies comprised randomised controlled trials (n=8), controlled clinical trials (n=2) and controlled before and after studies (n=5). Findings suggested that the addition of specialist nursing and specialist support roles to the nursing workforce may improve some patient outcomes. The authors found no evidence that the addition of specialist nurses reduces patient death rates, attendance at the emergency department, or readmission rates, but it is likely to result in shorter patient hospital stays and reductions in pressure ulcers. Specialist support staff, such as dietary assistants, may have an important impact on patient outcomes. The introduction of “primary nursing” and “self-scheduling” may reduce staff turnover. The authors concluded that, due to the limited evidence, the findings should be treated extremely cautiously. No suitable studies of interventions relating to nurse staffing levels, education mix, or grade mix were identified. The authors noted the need for larger, controlled studies.
Butler M, Collins R, Drennan J, Halligan P, O’Mathúna DP, Schultz TJ et al. Hospital nurse staffing models and patient and staff-related outcomes. Cochrane Database Syst Rev 2011; 7:CD007019.
https://doi.org/10.1002/14651858.CD007019.pub2
STUDY N (HS&DR 08/1819/215) PUBLISHED
Effectiveness of Multi-Professional Team Working (MPTW) in mental health care
Published, 2012, Principal Investigator West M
This mixed methods study aimed to identify the main factors in effective multi-professional team working in community mental health teams. The study had three stages. First, researchers held 10 workshops with service providers, users and carers (n=157 total participants), from 13 mental health trusts across England. These workshops informed the development of a questionnaire about team effectiveness. Second, researchers surveyed 135 community-based adult mental health teams across 11 NHS trusts, using this questionnaire and a team performance inventory (n=1500 team members responded, 67% response rate). Teams included those working with older adults, rehabilitation and recovery, early intervention, and generic teams. Third, researchers conducted in-depth studies of 19 teams, including observations of team meetings and interviews with staff (n=114), service users (n=31) and carers (n=13). Predictors of community mental health team effectiveness included: practical support for innovative approaches, team participation in decision making, regular meetings, trust, safety and support among team members, good team leadership, the right skills mix, effort, clarity of purpose and team objectives, promotion of carer involvement, organisational support and resources available, particularly staff availability. Limitations included service restructuring taking place during the research, and the questionnaire stage relying on data that team members self-reported.
West M, Alimo-Metcalfe B, Dawson J, El Ansari W, Glasby J, Hardy G et al. Effectiveness of Multi-Professional Team Working (MPTW) in mental health care. Final report. NIHR Service Delivery and Organisation programme; 2012.
https://www.journalslibrary.nihr.ac.uk/programmes/hsdr/081819215/#/
STUDY O (HS&DR 12/5004/01) PUBLISHED
Enhancing and Embedding Staff Engagement in the NHS: Putting Theory into Practice
Published, 2015, Principal Investigator Bailey K
This study reviewed existing evidence about staff engagement to find out whether people perform better at work and/or experience higher levels of wellbeing when they are engaged, and which workplace factors increase engagement. Researchers found 172 articles, published in peer-reviewed journals since 1990, that met their quality standards. They also evaluated 38 literature reviews and various practitioner materials. Overall, the evidence suggested that when people are engaged they tend to perform better, help colleagues more, and be more satisfied with their work and life in general. The researchers identified six factors linked to this: certain psychological states (such as resilience, self-efficacy and personal resources); people having the resources and tools needed to do their jobs; positive leadership; feeling supported by the organisation; working in a team with other engaged people; and taking part in training which boosts individuals’ coping strategies. However, the evidence was mixed; few studies focused on the healthcare sector, most used self-report surveys and only two took place in the UK. The term ‘engagement’ had many different meanings. The researchers concluded that there is a gap in knowledge about how engagement works in practice, and that further research is needed, particularly in the healthcare sector.
Bailey C, Madden A, Alfes K, Fletcher L, Robinson D, Holmes J et al. Evaluating the evidence on employee engagement and its potential benefits to NHS staff: a narrative synthesis of the literature. Health Serv Deliv Res 2015;3(26)
https://doi.org/10.3310/hsdr03260
STUDY P (HS&DR 08/1819/213) PUBLISHED
Patients’ experiences of care and the influence of staff motivation, affect and well-being
Published, 2012, Principal Investigator Maben J
This three-year mixed methods study explored links between patients’ experiences of healthcare, and the motivation, feelings and wellbeing of staff. Researchers conducted two patient focus groups, and interviewed 55 senior managers from two acute and two community NHS trusts in England. They selected two teams, wards or clinical units within each trust, in different care settings. They surveyed staff (n=427) and patients (n=498), interviewed staff (n=86) and patients (n=106), and observed day-to-day interactions, across the eight areas. They found that patient experiences were generally better when staff felt part of a good local team, experienced job satisfaction and a positive organisational climate, had low emotional exhaustion, and had support from co-workers, supervisors and the organisation. Ward/ team leaders played a critical role in setting expectations. Emotionally exhausting and demanding working environments, such as accident and emergency, negatively impacted on staff even when they were performing well. The researchers concluded that enhancing staff wellbeing is important both in its own right and for the quality of patient experiences. Recommendations included supporting staff to engage with patients on a meaningful personal level, regularly monitoring patient experience and staff wellbeing to target resources to problem areas, and disseminating good practice from highperforming teams.
Maben J, Peccei R, Adams M, Robert G, Richardson A, Murrells T et al. Patients’ experiences of care and the influence of staff motivation, affect and well-being. Final report. NIHR Service Delivery and Organisation programme; 2012
https://www.journalslibrary.nihr.ac.uk/programmes/hsdr/081819213#/
STUDY Q (HS&DR - 13/07/49) PUBLISHED
A realist informed mixed methods evaluation of Schwartz Center Rounds® in England
Published, 2018, Principal Investigator Maben
J Schwartz Center Rounds® aim to support healthcare staff to deliver compassionate care. They involve monthly group meetings where staff can safely reflect on the emotional, social and ethical challenges of care. This mixed methods study investigated how participation in Rounds affects staff wellbeing and patient care. Researchers mapped 77 Rounds providers in England in September 2014, rising to 115 by July 2015, of which three quarters were NHS trusts. Healthcare staff within 10 sites were surveyed before attending Rounds and eight months later. In all, 500 people responded at both time points, including regular attenders (n=51), irregular attenders (n=205) and non-attenders (n=233). In-depth case studies of nine organisations involved observations and 177 interviews. The survey found no change in engagement but a significant reduction in poor psychological wellbeing in regular Rounds attenders (25% to 12%) compared with nonattenders (37% to 34%). The authors identified a cumulative impact of Rounds. Reported outcomes included increased empathy and compassion for colleagues and patients, support for staff and changes in practice. Frontline staff could find it difficult to attend, and organisational support was required to sustain Rounds. Study limitations included outcomes relying on self-report and fewer regular attenders being recruited than desired.
Maben J, Taylor C, Dawson J, Leamy M, McCarthy I, Reynolds E, et al. A realist informed mixed methods evaluation of Schwartz Center Rounds® in England. Health Serv Deliv Res 2018;6(37)
https://doi.org/10.3310/hsdr06370
STUDY R (HS&DR - 14/194/21) ONGOING
Protocol published, 2016, Principal Investigator Griffiths P
The Safer Nursing Care Tool, widely used in the NHS, indicates the number of nurses required on a ward to meet patient need. This observational study will provide evidence for its usefulness and accuracy, and will model the costs and consequences of different staffing strategies aimed at addressing fluctuations in patients’ needs. The study will include all adult medical/surgical wards of one specialist and three general hospitals (n= 75 wards, over 1700 beds). Data on ward nurse staffing, validated nurse reported measures of staffing adequacy, and Safer Nursing Care Tool measures of patient needs, will be collected daily over a one-year period.
https://www.journalslibrary.nihr.ac.uk/programmes/hsdr/1419421/#/
STUDY S (HS&DR 14/194/20)PUBLISHED
Published, 2018, Principal Investigator Burton CR
This study investigated how NHS managers’ use of workforce planning and deployment technologies impacts on nursing staffing and patient care, and what works, for whom, how and in what circumstances. Such tools can help with the complex task of allocating staff effectively, complying with patient safety standards, forecasting demand, and communicating transparently about staffing. The tools rely on correct inputting and updating of data. The study comprised four phases. First, NHS managers, patient and public representatives and policy experts developed a theory about how the tools work in different contexts. Second, researchers reviewed existing evidence, guided by the theory. Third, interviews with NHS managers (n=11), a nurses’ Twitter chat, and an advisory group, helped refine the theory. Fourth, practical recommendations for managers were developed. The tools had a positive impact when they clearly combined data on needs and resources, when there was technical and leadership support, and when they were part of a collaborative process. Managers needed to combine local knowledge and professional judgement with data from the tools for effective staffing decisions. Study limitations included a lack of detailed evidence about how managers apply professional judgement. Most available evidence related to adult acute settings.
Burton CR, Rycroft-Malone J, Williams L, Davies S, McBride A, Hall B, et al. NHS managers’ use of nursing workforce planning and deployment technologies: a realist synthesis. Health Serv Deliv Res 2018;6(36)
https://doi.org/10.3310/hsdr06360
STUDY T (PHR 10/3007/06) PUBLISHED
Published, 2015, Principal Investigator Stansfeld SA
This pilot study tested the feasibility and acceptability of conducting a trial of an online learning program for managers to improve employee wellbeing and reduce sickness absence. It comprised a pilot cluster randomised controlled trial within a mental health NHS trust, in which three groups of employees and their managers were randomly allocated to receive the e-learning intervention and a fourth group did not. In-depth interviews, focus groups and observations accompanied the trial. Managers completed the e-learning program over 10 weeks, with a facilitator and two face-toface meetings. Outcome measures included recruitment and participation of employees and managers; acceptability of the intervention and trial; employee well-being; employee sickness absence data. In total, 424 employees and 41 managers were recruited. Employees completed work and health questionnaires before the intervention (n=350) and after (n=291). Only half of the managers (n=21) adhered to the intervention, completing at least three of six modules. Some managers reported insufficient time. The authors concluded that the intervention and trial were feasible to participants. The economic assessment was also feasible. A future trial might need to gain more support from senior managers, encourage managers to complete the intervention, strengthen the online program, and allow longer for it to work.
Stansfeld SA, Berney L, Bhui K, Chandola T, Costelloe C, Hounsome N et al. Pilot study of a randomised trial of a guided e-learning health promotion intervention for managers based on management standards for the improvement of employee wellbeing and reduction of sickness absence: The GEM Study (Guided E-learning for Managers). Public Health Res 2015;3(9)
https://doi.org/10.3310/phr03090
STUDY U (HS&DR 13/157/44) WAITING TO PUBLISH
Protocol published, 2017, Principal Investigator Robert G
This study investigated the 10-year impact of the ‘Productive Ward: Releasing Time to Care’ programme, introduced in 2007 to improve ward efficiency, and free nurse time for direct patient care. Informed by earlier research about initial take-up, the researchers surveyed all NHS acute trusts in England, and studied two wards in each of six acute trusts. They compared three earlier and three later adopters of the programme, and included medical, surgical and care of the elderly wards. Researchers analysed trust documents and data, conducted observations, and interviewed staff at all levels, patient representatives, and those who led the initial implementation.
https://www.journalslibrary.nihr.ac.uk/programmes/hsdr/1315744/#/
STUDY V (HS&DR - 13/07/87) WAITING TO PUBLISH, INTERIM PUBLICATIONS
Intentional rounding in hospital wards: What works, for whom and in what circumstances?
Interim publications, 2017-2018, Principal Investigator Harris R
Intentional rounding is a structured process whereby nurses conduct regular checks, usually hourly, with every patient using a standardised protocol. Most trusts in England introduced intentional rounding from 2012. This mixed methods study investigated the impact and effectiveness of intentional rounding in hospital wards on the organisation, delivery and experience of care. It explored the perspective of patients, their family members and staff. It examined this at three levels: national, service provider organisation, and individual ward/ unit. The study had four phases. First, a review of academic and policy literature with stakeholder consultation. Second, a national survey of all non-specialist NHS acute trusts in England. Third, in-depth case studies of six wards within three hospitals in England involving interviews with staff, patients and relatives, observations, and analysis of routinely collected ward outcome data and costs. Fourth, combining the study findings with input from stakeholders. Findings from the first phase literature review (n=44 papers) suggested a lack of clarity about the purpose of intentional rounding, and limited evidence of how it works in practice.
Sims S, Leamy M, Davies N, Schnitzler K, Levenson R, Mayer F et al. Realist synthesis of intentional rounding in hospital wards: exploring the evidence of what works, for whom, in what circumstances and why. BMJ Quality & Safety 2018;27(9):743- 757.
http://dx.doi.org/10.1136/bmjqs-2017-006757
https://www.journalslibrary.nihr.ac.uk/programmes/hsdr/130787/#/
References
Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH (2002) Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA 288:1987–93.
Aiken, L.H., Sloane, D.M., Bruyneel, L., Van den Heede, K., Griffiths, P., Busse, R., Diomidous, M., Kinnunen, J., Kózka, M., Lesaffre, E. and McHugh, M.D. (2014) Nurse staffing and education and hospital mortality in nine European countries: a retrospective observational study. The Lancet 383(9931), pp.1824-1830.
Aiken, L.H., Sloane, D.M., Ball, J., Bruyneel, L., Rafferty, A.M. and Griffiths, P. (2018) Patient satisfaction with hospital care and nurses in England: an observational study BMJ Open 8(1), p.e019189.
American Nurses Association’s National Database of Nursing Quality Indicators The National Database of Nursing Quality Indicators: http://ojin.nursingworld.org/MainMenuCategories/ANAMarketplace/ANAPeriodicals/OJIN/TableofContents/Volume122007/No3Sept07/NursingQualityIndicators.aspx
American Nurses’ Credentialing Center ANCC Magnet Recognition Program: https://www.nursingworld.org/organizational-programs/ magnet/
Ball. J.E., Pike, G., Griffiths, P., Rafferty, A.M and Murrells, T. (2012) RN4Cast Nurse Survey in England National Nursing Research Unit Report: https://www.kcl.ac.uk/nursing/research/nnru/publications/Reports/RN4Cast-Nurse-survey-report-27-6-12-FINAL.pdf
Ball, J.E., Murrells, T., Rafferty, A.M., Morrow, E. and Griffiths, P. (2014) ‘Care left undone’ during nursing shifts: associations with workload and perceived quality of care. BMJ Qual Saf 23(2), pp.116-125.
Ball, J. E., Bryuneel, L., Aiken, L. H., Sermeus, W., Sloane, D. M., Rafferty, A. M., Lindqvist, R., Tishelman, C., Griffiths, P. & Consortium, R. C. (2017) Post-operative mortality, missed care and nurse staffing in nine countries: A cross-sectional study. International Journal of Nursing Studies.
Bruyneel, L., Li, B., Ausserhofer, D., Lesaffre, E., Dumitrescu, I., Smith, H.L., Sloane, D.M., Aiken, L.H. and Sermeus, W. (2015) Organization of hospital nursing, provision of nursing care, and patient experiences with care in Europe Medical Care Research and Review 72(6), pp.643-664.
Buchan, J., Seccombe, I., Gershlick, B, and Charlesworth, A (2017) In short supply: pay policy and nurse numbers London: The Health Foundation.
Carter, P. (2016) Operational productivity and performance in English NHS acute hospitals: Unwarranted variations: https://assets.publishing.service.gov.uk/government/uploads
/system/uploads/attachment_data/file/499229/Operational_productivity_A.pdf
Cookson, G., Jones., S., van Vlymen, J., and Laliotis, I. (2014) The Cost-Effectiveness of Midwifery Staffing and Skill Mix on Maternity Outcomes: https://www.nice.org.uk/guidance/ng4/evidence/economicevaluation- report-5277277
Department of Health, Social Services and Public Services (DHSSPS) (2014) Delivering Care: Nurse Staffing in Northern Ireland: https://www.publichealth.hscni.net/sites/default/files/dc-section1[1]%20FINAL%20PDF_0.pdf
Dixon, J., Street, A. and Allwood, D., 2018. Productivity in the NHS: why it matters and what to do next. BMJ 363, p.k4301.
Doyle, C., Lennox, L. and Bell, D., 2013. A systematic review of evidence on the links between patient experience and clinical safety and effectiveness. BMJ open, 3(1), p.e001570.
Fitzsimons B, Goodrich J, Bennett L and Buck D (2014). Evaluation of King’s College Hospital Volunteering service Final report: https://media.nesta.org.uk/documents
/kings_fund_evaluation_of_kch_impact_volunteering.pdf
Galletta, M., Portoghese, I., Battistelli, A. and Leiter, M.P. (2013) The roles of unit leadership and nurse–physician collaboration on nursing turnover intention. Journal of Advanced Nursing, 69(8), pp.1771-1784.
Griffiths, P., Ball, J., Drennan, J., James, L., Jones, J., Recio, A., and Simon,. (2014) The association between patient safety outcomes and nurse/healthcare assistant skill mix and staffing levels and factors that may influence staffing requirements Southampton, GB. University of Southampton.
Griffiths, P., Recio-Saucedo, A., Dall’Ora, C., Briggs, J., Maruotti, A., Meredith, P., Smith, G.B., Ball, J. and Missed Care Study Group (2018) The association between nurse staffing and omissions in nursing care: a systematic review Journal of Advanced Nursing 74(7):1474-1487.
Halter M., Boiko, O., Pelone, F., Beighton, C., Harris, R., Gale, J., Gourlay, S and Drennan, V. (2017a) The determinants and consequences of adult nursing staff turnover: a systematic review of systematic reviews BMC Health Services Research 17:824.
Halter, M., Pelone, F., Boiko, O., Beighton, C., Harris, R., Gale, J., Gourlay, S., and Drennan, V. (2017b) Interventions to reduce adult nursing turnover: a systematic review of systematic reviews The Open Nursing Journal 11 (2017b): 108.
Hayward, D., Bungay, V., Wolff, A.C. and MacDonald, V. (2016) A qualitative study of experienced nurses’ voluntary turnover: learning from their perspectives. Journal of clinical nursing, 25(9-10), pp.1336-1345.
Heinen, M.M., van Achterberg, T., Schwendimann, R., Zander, B., Matthews, A., Kózka, M., Ensio, A., Sjetne, I.S., Casbas, T.M., Ball, J. and Schoonhoven, L. (2013) Nurses’ intention to leave their profession: a cross sectional observational study in 10 European countries. International Journal of Nursing Studies 50(2), pp.174-184.
Hoffart, N. and Woods, C.Q. (1996) Elements of a nursing professional practice model. Journal of professional nursing 12(6), pp.354-364.
Jarman, B., Gault, S., Alves, B., Hider, A., Dolan, S., Cook, A., Hurwitz, B. and Iezzoni, L.I. (1999). Explaining differences in English hospital death rates using routinely collected data. BMJ 318(7197), pp.1515-1520.
Kitson, A. L., Wiechula, R. J., Conroy, T. A., MuntlinAthlin, A., & Whitaker, N. L. (2013). The future shape of the nursing workforce: a synthesis of the evidence of factors that impact on quality nursing care: https://digital.library.adelaide.edu.au/dspace/bitstream/2440/77059/1/hdl_77059.pdf
Lalfond S, Charlesworth A. (2017) A year of plenty? London: The Health Foundation.
Maben, J., Morrow, E., Ball, J., Robert, G., and Griffiths, P. High Quality Care Metrics for Nursing (2012) National Nursing Research Unit, King’s College London: https://eprints.soton.ac.uk/346019/1/High-Quality-Care-Metrics-for-Nursing----Nov-2012.pdf
Mid Staffordshire NHS Foundation Trust Public Inquiry (2013). Report of the Mid Staffordshire NHS Foundation Trust public inquiry—Executive summary: https://webarchive.nationalarchives.gov.uk/20150407084231 http://www.midstaffspublicinquiry.com/report
NHS Digital (2018a) NHS Workforce Statistics March 2018: https://files.digital.nhs.uk/EF/316A87
/NHS%20Workforce%20Statistics%2C%20March%202018%20Bulletin.pdf
NHS Digital (2018b) NHS Workforce Statistics - September 2018: https://digital.nhs.uk/data-and-information/publications/statistical/nhs-workforce-statistics/september-2018#keyfacts
National Quality Board (2014) How to ensure the right people, with the right skills, are in the right place at the right time: https://www.england.nhs.uk/wp-content/uploads/2013/11/nqb-how-to-guid.pdf
National Quality Board (2016) Supporting NHS providers to deliver the right staff, with the right skills, in the right place at the right time: https://www.england.nhs.uk/wp-content/uploads/2013/04/nqb-guidance.pdf
National Institute for Health and Care Excellence (2014) Safe staffing for nursing in adult inpatient wards in acute hospitals: https://www.nice.org.uk/guidance/sg1/chapter/3-Gaps-in-theevidence
Needleman, J., Buerhaus, P., Mattke, S., Stewart, M. and Zelevinsky, K. (2002) Nurse-staffing levels and the quality of care in hospitals New England Journal of Medicine 346(22) p.1715-1722.
Nursing and Midwifery Council (2019) Nursing Associates: https://www.nmc.org.uk/standards/nursing-associates/
Nursing Commission’s Report (1932) The Lancet 219: 5660 pp409.
Office of National Statistics (2016) UK Health Accounts: 2016: https://www.ons.gov.uk/peoplepopulationandcommunity/
healthandsocialcare/healthcaresystem/bulletins/ukhealthaccounts/
2016#total-current-healthcare-expenditure-in-the-uk
Petit, O.P. and Regnaux, J.P. (2015) Do Magnet accredited hospitals show improvements in nurse and patient outcomes compared to non-Magnet hospitals: a systematic review. JBI database of systematic reviews and implementation reports, 13(6), pp.168-219.
Porter, J., Ottrey, E. and Huggins, C.E. (2017) Protected Mealtimes in hospitals and nutritional intake: Systematic review and meta-analyses. International Journal of Nursing Studies, 65, pp.62-69.
Ross, S., Fenney, D., Ward, D. and Buck, D. (2018) The role of volunteers in the NHS: Views from the front line London: The King’s Fund: https://www.kingsfund.org.uk/publications/role-volunteers-nhs-views-front-line
Royal College of Nursing (2018) Fund our future nurses – Cost effective options to support nursing students and grow the nursing workforce in England London: RCN.
Twigg, D., Myers, H., Duffield, C., Pugh, J., Gelder,L. and Roche, M. The impact of adding assistants in nursing to acute care hospital ward nurse staffing on adverse patient outcomes: An analysis of administrative health data. International Journal of Nursing Studies 63 (2016): 189-200.
UKCC (1986) Project 2000: A new preparation for practice London: UKCC.
Welsh Government (2016) Nurse Staffing Levels (Wales) Act 2016 Statutory Guidance: https://gweddill.gov.wales/docs/phhs/publications/171102nurse-staffingen.pdf
Westbrook, J.I., Li, L., Hooper, T.D., Raban, M.Z., Middleton, S. and Lehnbom, E.C. (2017) Effectiveness of a ‘Do not interrupt’ bundled intervention to reduce interruptions during medication administration: a cluster randomised controlled feasibility study BMJ Qual Saf 26:734-742.
Wood, V.J., Vindrola-Padros, C., Swart, N., McIntosh, M., Crowe, S., Moris, S. and Fulop, N.J. (2018) One to one specialling and sitters in acute care hospitals: A scoping review. International Journal of Nursing Studies 84:61-77.
World Health Organisation (2018) Nursing and Midwifery Fact Sheet: https://www.who.int/mediacentre/factsheets/nursing-midwifery/en/
Glossary
Acuity: Acuity is the degree to which a patient has severe and recent onset symptoms which need prompt medical attention
Assistant Practitioner: Assistant practitioners (sometimes known as associate practitioners) have skills and experience in a particular area of clinical practice. Although they are not registered professionals they have a high level of skill through their experience and training (usually a Foundation Degree)
Healthcare Assistant: Healthcare assistants work under the guidance of a qualified healthcare professional, usually a nurse. Sometimes staff working in HCA roles are known as nursing assistants, nursing auxiliaries or auxiliary nurses
Intentional Rounding: Intentional rounding is a structured approach whereby nurses conduct checks on patients at set times to assess and manage their fundamental care needs
Lean management: A system for developing process improvement that focuses on reducing and eliminating waste
Licensed Practical Nurse: Licensed Practical Nurse is a regulated role in many countries (although not the UK). They undertake training of one or two years and are responsible for providing fundamental nursing care and usually work under the supervision of registered nurses
Nursing Associate: A nursing associate is a role in the UK that will provide care and support for patients and service users. It is intended to address a skills gap between health and care assistants and registered nurses
Observational studies: Studies which are not experimental, but where individuals and populations are observed and associations made between different variables
Physician Associates: Physician Associates are graduates who have undertaken post-graduate training and work under the supervision of a medical practitioner
Registered Nurse: A Registered Nurse is a nurse who has met the criteria for a nursing license defined by their country’s statute. They are independently accountable for their decisions and actions
Roster: A list or plan showing turns of duty or leave for individuals
Schwartz Round: Schwartz rounds are a forum for hospital staff from all backgrounds to come together to talk about the emotional and social challenges of caring for patients. The aim is to offer staff a safe environment in which to share their stories and offer support to one another
Specialling: One-to-one observation to reduce the risk and incidence of harm to the patient
Ward Climate: The ward climate is the sense, feeling or atmosphere people get on a day-to-day basis. It differs from culture which is defined as the (often unconscious) pattern of shared basic assumptions that direct the way the ward works
Workforce planning and deployment technologies: Tools to assist workforce planning and help make better decisions about cost effective numbers and mixes of staff. Usually derived from statistical analysis of past staffing and/or benchmarking
Work processes: Work processes are the set of steps or tasks used in the ward to achieve a specific goal
Acknowledgements
This report was written by Elaine Maxwell, with Katharine Hanss and Tara Lamont of the NIHR Dissemination Centre.
Expert input was provided by a steering group consisting of:
- Jane Ball Professorial Research Fellow, University of Southampton
- Ron Capes Lead Governor, Basildon and Thurrock University Hospitals NHS FT
- Lara Carmona Associate Director of Policy and Public Affairs, Royal College of Nursing
- Howard Catton Chief Executive of International Council of Nurses
- Anita Charlesworth Director of Research and Economics, The Health Foundation
- Sue Covill Director of Development and Employment, NHS Employers
- Vari Drennan Professor of Health Care and Policy Research, Kingston and St George’s University
- BevFitzsimmons Head of Improvement, Point of Care Foundation
- Sam Foster Chief Nurse, Oxford University Hospitals NHS Foundation Trust
- Peter Griffiths Chair of Health Services Research, University of Southampton
- John Jones Lead Governor, Essex Partnership University NHS Foundation Trust
- Alison Leary Chair of Healthcare and Workforce Modelling, London South Bank University
- Jane Noyes Professor in Health & Social Services, Bangor University
- Mark Radford Director of Nursing (Improvement), NHS Improvement
- Janice Smyth Director, Northern Ireland Royal College of Nursing
- Karen Spilsbury Chair in Nursing Research, University of Leeds
NIHR Dissemination Centre launched its themed review Staffing on Wards on 26th March at Hammersmith Hospital. An invited audience of 80 people listened to presentation about the evidence and held table discussions about the implications of the research evidence.
Below, we present a summary of those conversations and recommendations here and invite comments about the next steps needed to translate the findings into practice.
View the slides from the day:



As a Director of Nursing achieving good quality outcomes for patients is my main priority. In the complex times we work in it’s vital that we understand what the evidence tells us in relation to nurse staffing and quality of care. As the professional advisor to my Board this review helps me to advise the Board, with certainty, what staff we need to assure high quality care. One of the most interesting findings was the important relationship between registered and unregistered staff and the ratios that lead to the best outcomes.
Juliette Cosgrove, Director of Nursing, Midwifery and Therapies at Southport and Ormskirk Hospital NHS Trust
The NIHR Themed Staffing Review was an extremely insightful and stimulating event, providing useful evidence to inform and assist nursing leaders reflect on workforce challenges and maximise current staffing resources and practices more effectively.
Heather Finlay, Nursing Officer at the Department of Health Northern Ireland
Table discussions summarised:
Strength of the evidence
The meeting felt that the science around ward staffing is imperfect (although significantly better than for any other part of the workforce) although there was an understanding that RCTs would not be possible for many workforce questions. However, there are strong and consistent messages in the review that should form the basis for policy and action unless and until more evidence emerges.
The challenge is to ensure the research is well understood from ward to board. The research clearly identifies a ‘sweet spot’ for registered nurse hours but there are many intervening variables, including the ward climate and the way nurses are deployed and managed and the changing shape of multi professional teams. These vary significantly between wards and between hospitals.
It is not clear whether a universal minimum number of registered nurses for all wards can be determined from the evidence, and some fear such a figure becoming the norm rather than a safety net. The research does not present a binary choice of safe/unsafe. There is a focus on tasks completed and harms rather than assessment and decision making to promote excellent care. Understanding the degrees of risk should inform actions when the best practice is not possible due to lack of funding or lack of supply of staff.
Research joining up the numbers and the conditions is needed. For example, is it better to fill an absence on the roster with an HCA who knows the ward well and is part of a well-functioning team or to employ an Agency or Bank Registered Nurse who has not worked on the ward before? The most surprising evidence for many of the delegates was the U shaped relationship between the number of HCAs and patient harms which was described as ‘counter intuitive’. For others, the most surprising evidence was the clear impact of the ward environment and staff welfare on patient as well and staff satisfaction.
Increase research literacy and dissemination
Staffing on wards is complex and utilising the evidence well requires a degree of research literacy. It was suggested that Nurse Directors need to role model reflection on research findings. This includes translation of the research and its application to local needs, including the different types of wards within a hospital. Practice development teams could be well placed to disseminate research findings. There was support for dedicated dissemination resources for Chief Nurses and a suggestion that research be presented as problem solving, using a ‘You asked, we discovered’ campaign.
Governance and assurance
The strong messages in the evidence need to be embedded in each organisation’s governance and assurance systems, starting with commissioners’ of services. There was a call for workforce requirements to be transparent in contracts, with contingencies for the workforce required for additional work. For governance and assurance, the evidence needs to be presented in ways that make risk and consequence more explicit and it was felt that NHS England/Improvement could have a role in developing a nursing assurance toolkit which could be used by commissioners, regulators and providers ( as they have with Friends and Family test, MRSA reporting etc). Such an assurance tool would be required to join the dots between fill rates, harms, retention of staff and ward climate and patient experience.
Analytics
One of the challenges of acting on the evidence base is the lack of local analysis of real time data. The evidence can be used to make optimal decisions if providers can model different staffing configurations based on demand and staff availability. Local cost modelling with predicted risks could inform both Board decision making and managing the daily flux of supply and demand. The existing available data could inform decision but staff will need coaching on how to use it.
Board accountability
Most Boards currently receive monthly reports of ward staffing fill rates without wider indicators. It was felt that Boards understand the financial spend without a full understanding of risks and benefits and that there needs to be greater transparency in the Boards’ accountability. It was perceived that ward staffing was determined from the allocated funding rather than from an understanding and acceptance of the level of risk.
Leadership
Leadership at all levels of organisations was seen to be key to translating the evidence into useful operational guidance. This was felt to require investment in nurse leadership development, both for determining and managing the shape of the ward team and for creating and maintaining good ward climates. This would include writing and presenting business cases, using local data to understand the impact of day to day flux as well as creating supportive environments and managing staff.
Systems and team thinking
Some delegates encouraged colleagues to think about wards staffing as part of a wider system, both within a hospital and across an integrated care system. The lack of evidence outside hospital wards should not mean that these areas are overlooked and resources focused on hospitals. The evidence on registered nurse and HCAs should not prevent integration with other professions where it is safe to do so. This requires clarity about the role and value of registered nurses in multidisciplinary teams. Unregistered staff and volunteers have a role to play but should be deployed in line with the evidence and have clear boundaries with registered practitioners.
The evidence on the importance of team work was welcomed but delegates cautioned that it cannot compensate for structural problems (including staff shortages). Considering the staffing needs across multi professional teams can be challenged by operational silos and separate budgets. More understanding of professional overlaps and interdependencies is required. Evidence is needed on the impact of new support roles such as Nursing Associates, particularly how this interfaces with the evidence on registered nurse requirements.
Creating the environment for maximising staff effectiveness
The strength of the evidence around managing emotional labour was new to some and delegates wanted to consider practical actions that increase the resilience of both teams and individuals. Some suggested that there is a vicious circle that when there is inadequate staffing, maintaining staff welfare and ward climate becomes more challenging. Some delegates thought that the evidence on teamwork suggests that moving the available staff to different wards may be counterproductive and lead to more stress and more staff leaving. Where teams having changing membership, team leaders need help to develop skills to manage them well.
The evidence around lack of time and physical space (for example, the loss of staff rooms) for reflection and team building resonated with delegates, who thought time for reflection and supervision should be built into calculation of staffing hours.
Staff supply
The discussion focused around the supply for registered nurses. It was felt that the evidence around staffing requirement for safe and effective care had not been used to inform strategic workforce planning, which had been based on historic patterns. Current campaigns to attract more people to study nursing should use the evidence on the impact registered nurses have on outcomes and safety and not focus on caring alone.
Recruiting more entrants without retaining more staff is self-defeating and organisations should be required to report on how they are using the evidence to improve ward climates and retain staff. Delegates felt that sabbaticals after a fixed number of years would help to retain more experienced staff.
Using local data, organisations can predict their own short and medium term supply requirements and should over recruit when students graduate to ensure they do not incur long term vacancies.
Building on the evidence around staff welfare, organisations should create a new range of career pathways where nurses can combine clinical practice with either managerial or academic responsibilities. Technology should be explored to enhance nursing care but is unlike to replace nurses.
Conclusion
Participants found the research stimulating and helped them to reflect on current practices and challenges. While supply issues dominate day to day work, many good ideas emerged during the discussion that could enhance staff retention and create safe and supportive environments. There was interest and demand for research and delegates expressed a need for time to absorb and make sense of evidence and best practice.
They was an appetite for resources to help staff at all levels to understand and share the evidence. This might include a slide deck for sharing the findings of our review and a nursing assurance toolkit. Please let us know your thoughts on this and on any part of the discussion.
Produced by the University of Southampton on behalf of NIHR through the NIHR Dissemination Centre